
Body
Spinal cord injury (SCI) can be life-changing for patients — and, after injury, patients and their families often are faced with a flood of unfamiliar medical terms that can be overwhelming.
However, understanding common terms surrounding SCI helps patients make informed decisions and take a more active role in their care, rehabilitation and long-term healing.
To help patients navigate their recovery, Shirley Ryan AbilityLab offers a guide to terminology about SCI:
Spinal Cord Injury
Body
A spinal cord injury (SCI) occurs when there is damage to the spinal cord, resulting in a loss of function, such as mobility or sensation.
The spinal cord — a long, thin bundle of nerves that extends from the brainstem down through the spinal column — acts as the main communication highway between the brain and the rest of the body. When this pathway is disrupted, it can affect the body’s ability to move or feel below the level of injury.
Commonly, SCI is caused by a traumatic injury, such as a car accident, a fall, sports injury or trauma, such as from a gunshot wound. Infections, tumors or degenerative diseases also can damage the spinal cord.

Complete vs. Incomplete Spinal Cord Injury
Body
A spinal cord injury is distinguished by its severity: complete or incomplete. This determination is important for patients to have a full understanding of their prognosis and potential for recovery.
- A complete SCI means there is a total loss of sensory and motor function below the level of injury, as the brain cannot send or receive signals past the point of damage. As a result, patients experience full paralysis and loss of sensation below the injury. While the damage is irreversible in a complete SCI, rehabilitation can help patients maximize their function and improve their quality of life.
- An incomplete SCI means some communication still exists between the brain and the areas below the injury. This may result in partial movement or sensation. The extent of function varies widely and depends on the severity and location of the injury. However, many patients with incomplete SCI make significant progress through rehabilitation — recovering lost abilities and regaining function, such as mobility.
Tetraplegia (Quadriplegia) vs. Paraplegia
Body
Many patients experience paralysis due to an SCI. The terms tetraplegia (also known as quadriplegia) and paraplegia describe the extent of the paralysis.
- Tetraplegia (quadriplegia) refers to paralysis that affects all four limbs, as well as the torso. It usually results from an injury to the cervical (neck) portion of the spinal cord. People with tetraplegia may experience varying degrees of impairment in their arms, hands, trunk and legs. In severe cases, they may also have difficulty speaking, swallowing and/or breathing on their own.
- Paraplegia refers to paralysis that affects the lower half of the body, typically the legs and lower torso. It usually results from injury to the thoracic lumbar or sacral regions of the spinal cord. Individuals with paraplegia retain full use of their arms and hands, but may have difficulty walking or may be unable to walk at all.
Types of Spinal Cord Injury by Location
Body
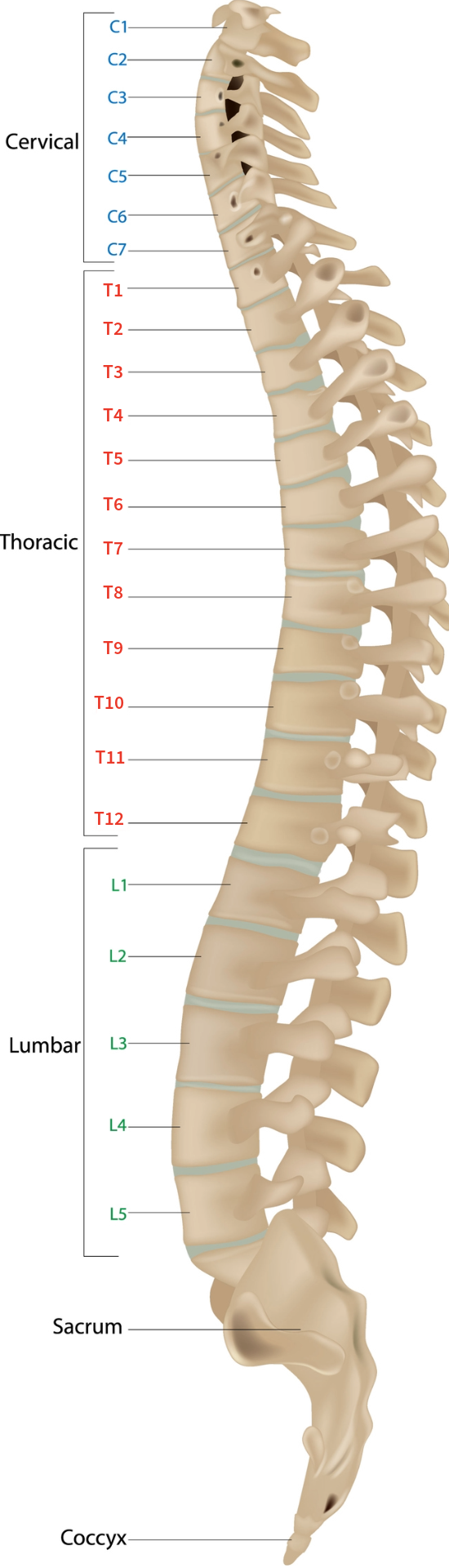
The location of the injury on the spinal cord plays a major role in determining which parts of the body are affected. The spinal cord is divided into four main regions:
Body
 |
|
SCI & Rehabilitation
Body
By knowing the severity of an SCI, where the injury is located on the spinal cord, and the extent of paralysis and/or impairments, medical teams can tailor treatment plans and set SCI rehabilitation goals with patients. In many cases, a comprehensive, interdisciplinary approach — such as SCI rehabilitation offered at Shirley Ryan AbilityLab — offers patients the best chance of recovery.
For example, a patient with limited use of their arms or hands may benefit from coordinated physical and occupational therapy to regain upper-body strength and rebuild fine-motor skills. A patient with leg impairments may need to learn how to use a wheelchair, or learn to walk with the assistance of a walker or orthotics (braces). Also, speech therapy can help patients recover communication skills or cognitive function, while swallow therapy can help patients learn to swallow safely and eat and drink independently after injury or paralysis.
